Natalie Davies

Natalie Davies is content manager for the Society for the Study of Addiction website, and co-owner of Drug and Alcohol Findings, an archive of over a thousand analyses of drug and alcohol interventions. She has a master’s degree with distinction in Women’s Studies, and has a particular interest in studying reproductive rights and violence against women from a feminist perspective. In September 2021, Natalie produced The Pregnancy Edit – a collection of articles and resources on alcohol-related harm in pregnancy, published on the Society for the Study of Addiction website.
While there is no evidence to suggest that women need to avoid alcohol altogether in order to get pregnant or have a healthy pregnancy, expert bodies in the UK recommend total abstinence from alcohol for women who are trying to conceive and women who are already pregnant (British Medical Association, 2016; Department of Health, 2016; Royal College of Obstetricians and Gynaecologists, 2018).
The following essay will explore the implications of this advice for women who are trying to conceive – a group which has tended to be neglected in discussions about pregnancy and alcohol consumption – and furthermore will suggest that there may be an alternative to the abstinence-based approach that can integrate alcohol harm reduction with family planning.
Alcohol guidelines for the general and ‘childbearing’ population
A study published in The Lancet found that there is no universally safe level of alcohol consumption. Its authors concluded that “the safest level of drinking is none”; people differ physiologically, and a ‘safe’ level of alcohol for one person might harm another (GBD 2016 Alcohol Collaborators, 2018). There is, however, a recognised need to make generalisations about where alcohol consumption can pose a low versus a high risk of harm, in order to try and reduce harm across the population.
Drinking guidelines for the general population support adults to make informed choices about their drinking. While they do not encourage people to drink, they also do not expect that people will abstain from alcohol. Up until 2016, the same principle was applied to the ‘childbearing’ segment of the population too. Thereafter, the official message for women who are pregnant, women who could get pregnant, and women who are breastfeeding was that ‘the safest approach is not to drink any alcohol’.
The change in focus from trying to reduce alcohol-related harm among women in and around the time of pregnancy, to trying to eliminate any risk of harm, was ostensibly guided by two things: increasing concern about fetal alcohol spectrum disorders, a group of lifelong behavioural, cognitive and physical disabilities caused by exposure to alcohol before birth (Mukherjee, 2018); and, the conviction of public health experts that women “need […] clarity and simplicity” in alcohol guidance (Department of Health, 2016). It was not, as one might expect, underpinned by evidence that any alcohol can harm a pregnancy, or indeed evidence of the effectiveness of abstinence messages for reducing alcohol-related harm.
The decision by the British Medical Association (2016), Department of Health (2016), and Royal College of Obstetricians and Gynaecologists (2018) to encourage women to abstain from alcohol was a well-intentioned response to harms that everyone would like to avoid. However, even well-meaning advice can fail to respond to the needs and experiences of women, and in this context, advice to abstain may be letting women down in several crucial ways.
- The advice excludes the possibility of harm reduction. Clinical guidelines on substance use problems recommend pragmatic and evidence-based interventions to reduce harm where people continue to use potentially harmful illicit drugs (Department of Health, 2017); in the same way, a harm reduction approach could support women to reduce the risk to themselves and their pregnancies should they continue to drink.
- The advice does not reflect the evidence base. UK guidelines from the Chief Medical Officers are reportedly underpinned by the principles that “people have a right to accurate information and clear advice about alcohol and its health risks”, and the “government has a responsibility to ensure this information is provided for the public in a clear and open way, so they can make informed choices” (Department of Health, 2016). While there is no evidence to suggest that light drinking during pregnancy can cause harm to the developing embryo/fetus, categorical advice to abstain from alcohol may give the impression that any and all drinking is inherently harmful.
- The advice is paternalistic. Whereas the rest of the adult population are supported to make an informed choice about their drinking, women in the ‘childbearing’ category are supported only to make the ‘right’ choice (Brown and Trickey, 2017).
- The advice can produce unintended consequences. Women attending healthcare clinics run by the British Pregnancy Advisory Service have disclosed wanting to terminate their pregnancies for fear that drinking early in pregnancy caused irrevocable harm (Davies, 2021).
Responding to the needs of different groups of women
UK drinking guidelines put women who are trying to conceive in the same category as women who are already pregnant, despite these two groups of women being in a materially different situation, with potentially very different concerns or priorities for their lives.
Trying to conceive is not a guarantee of pregnancy, and certainly not an assurance that pregnancy will happen soon. The NHS website says that 92% of women aged 19 to 26 will conceive after one year, and 98% will conceive after two years. For women aged 35 to 39, 82% will conceive after one year and 90% will conceive after two years (NHS, 2018a).
For many women, that one or two years of trying to conceive is not one or two years of knowing that they will get pregnant. It may be one or two years wondering whether they will ever get pregnant, and agonising over whether they have undiagnosed infertility issues. It may be month after month of negative pregnancy tests and buying more period products. It may be worrying that, even if they do get pregnant, theirs will be the one in five of all pregnancies that ends in a miscarriage in the first three months (British Pregnancy Advisory Service, n.d.).
Expecting women to behave as if they are pregnant before they are pregnant, and without any guarantee that they will ever be pregnant, increases the emotional burden on women of trying to conceive. Assuming that a woman’s only reference point for making decisions is the health of her hypothetical or future embryo/fetus reduces her purpose and outlook to the act of procreation. Branding alcohol consumption during this time as ‘risky behaviour’ stigmatises women and ignores the beneficial role that alcohol can play for women who are trying to conceive, including drinking for relaxation, drinking for pleasure, and drinking to cope with the consequences or symptoms of sexual trauma.
Integrating harm reduction with family planning
The primary impetus for recommending abstinence among women who are trying to conceive is to try and prevent alcohol consumption in what is known as the ‘pre-recognition period’ (the days or weeks between conception and confirmation of pregnancy). However, there may be other ways of preventing alcohol-related harm in the pre-recognition period, besides abstinence. For example, there are some basic rules about the menstrual cycle that can help women to maximise their chances of conceiving, and also help women to zero in on the pre-recognition period if they are concerned about inadvertently drinking in early pregnancy, or are concerned about alcohol-related harm in early pregnancy from drinking heavily.
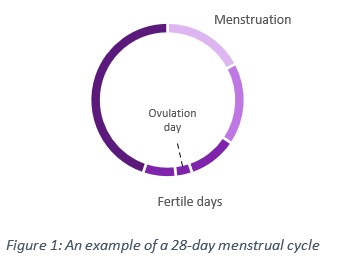
Figure 1 illustrates a typical 28-day cycle, including the days in the month when women could expect to menstruate, and the day when they could expect to ovulate. It is not an exact science because women’s bodies are all different, and women’s cycles may not be consistent from one month to the next. However, this type of information is already available to women and is being used by many women for the purposes of family planning (i.e. planning or avoiding pregnancy).
Women are most fertile on the days around ovulation, so, armed with this information, women who want to get pregnant may track their cycles and time sexual intercourse in order to maximise their chances of conception, although this is not currently recommended by the NHS.
Women may be able to build a more accurate picture of their menstrual cycles by using tools such as:
- Ovulation tests: These work by identifying the hormone surge that occurs just before an egg is released from one of the ovaries.
- Period tracker apps: These can be installed on mobile phones, and work by women inputting data about events in their menstrual cycles, such as the start and end of their period. Typically, the predictions about the date of ovulation and the start of a woman’s next period will become more accurate over time as women continue to input data month after month. Period tracker apps enable women to forecast what days during the month they will have a low, medium, or high chance of getting pregnant.

Current guidelines advise women who are trying to conceive to completely abstain from alcohol, and Figure 2 maps this categorical advice onto a 28-day cycle. As the red ring highlights, the serious message conveyed to women is: drink alcohol and risk immense harm; abstain from alcohol and have zero risk of harm.
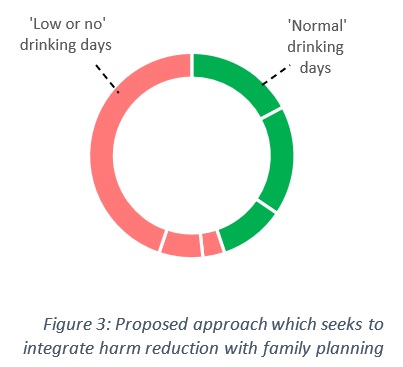
Figure 3 demonstrates an alternative to abstinence, whereby women could opt to have ‘normal drinking’ days from the first day of their period to ovulation, and adopt ‘low or no drinking’ days from ovulation to the first day of their next period (or until they confirm that they are not pregnant). Rather than 28 days of every month not drinking, this integrated alcohol harm reduction and family planning approach would translate into a hypothetical 13 out of 28 days as normal drinking days, and 15 out of 28 days as low or no drinking days.
This type of intervention could be delivered in a number of ways, including via official guidance, professional advice, and self-education. It would also translate very well into a mobile phone app – much like existing period tracker apps, but with additional functionality to inform women when they could opt for a normal drinking day versus a low or no drinking day.
Compared with the abstinence-based approach in current guidelines, the proposed approach could offer a number of potential benefits. For example, it could support women to be mindful about their drinking. It could enable women to minimise the risk of alcohol-related harm in the pre-recognition period, should they get pregnant, while also being able to continue with the rest of their lives. It could enable women to integrate harm reduction with their goal of trying to conceive. It could alleviate guilt and shame by allowing women to determine what a ‘normal’ drinking day is versus a ‘low’ drinking day, rather than measuring themselves against a target that is difficult or impossible to meet. And, it could give women real choices about their drinking and the ability to change their minds, as opposed to a binary choice between the ‘right’ way of doing something and the ‘wrong’ way of doing something at a single point in time.
Researching the needs and experiences of women who are trying to conceive
There are many dimensions to the issue of preventing alcohol-related harm in and around pregnancy. Research avenues that have been explored to date include perceptions of abstinence-only drinking guidelines for pregnant women (e.g. Brown and Trickey, 2018), as well as levels of alcohol consumption and attitudes towards drinking during pregnancy (e.g. Mardby et al., 2017).
The DECIPHer project, for example, examined the implications of UK alcohol guidelines for pregnant women. Dr. Rachel Brown and Dr. Heather Trickey talked to different groups of stakeholders and found that the lack of nuance in alcohol guidelines sometimes led women to mistrust the advice. Furthermore, they found that there were consequences to women complying with the abstinence message, which could include women tacitly revealing their pregnancy before they were ready by saying no to a drink in a social situation. Especially pertinent to this essay, the DECIPHer project also found that guidance to abstain from drinking while pregnant or planning a pregnancy was incompatible with women’s lives, particularly within a culture where social drinking is normal (Brown and Trickey, 2018).
There is a discernible need to build on this key piece of work, and examine the way that women who are trying to conceive make sense of and engage with alcohol guidelines. As this essay sought to show, women who are trying to conceive are a group distinct from women who are already pregnant. They have materially different needs and considerations, including the fact that pregnancy – however desired this outcome is – is never guaranteed. The alternative to abstinence that was proposed within this essay aimed to show that innovative interventions for reducing harm in and around pregnancy are possible when the needs and experiences of women are centred. The opportunity here is to start listening to these needs and experiences.
References
- British Medical Association (2016). Preventing and managing fetal alcohol spectrum disorders. https://www.bma.org.uk/what-we-do/population-health/supporting-people-to-live-healthier-lives/reducing-alcohol-related-harm-in-england
- British Pregnancy Advisory Service (n.d.). Miscarriage care. https://www.bpas.org/more-services-information/miscarriage-care/
- Brown and Trickey (2018). Communicating public health alcohol guidance for expectant mothers: a scoping report. https://alcoholchange.org.uk/publication/communicating-public-health-alcohol-guidance-for-expectant-mothers-a-scoping-report-1
- Davies (2021). The WRISK project: Understanding and improving the way risk in pregnancy is communicated to women. https://www.addiction-ssa.org/the-wrisk-project-understanding-and-improving-the-way-risk-in-pregnancy-is-communicated-to-women/
- Department of Health (2016). UK Chief Medical Officers’ low risk drinking guidelines. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/545937/UK_CMOs__report.pdf
- Department of Health (2017). Drug misuse and dependence: UK guidelines on clinical management. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/628634/clinical_guidelines_2017.pdf
- Department of Health (2017). UK Chief Medical Officers’ Alcohol Guidelines Review: Summary of the proposed new guidelines. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/489795/summary.pdf
- GBD 2016 Alcohol Collaborators (2018). Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. https://doi.org/10.1016/S0140-6736(18)31310-2
- Mardby et al. (2017). Consumption of alcohol during pregnancy – a multinational European study. https://doi.org/10.1016/j.wombi.2017.01.003
- Mukherjee (2018). A cup half full or half empty? A reflection on 15 years working with Fetal Alcohol Spectrum Disorders (FASD) in the UK. https://www.acamh.org/blog/fasd/
- NHS (2018a). How long does it usually take to get pregnant? https://www.nhs.uk/pregnancy/trying-for-a-baby/how-long-it-takes-to-get-pregnant/
- Royal College of Obstetricians and Gynaecologists (2018). Alcohol and pregnancy. https://www.rcog.org.uk/globalassets/documents/patients/patient-information-leaflets/pregnancy/pi-alcohol-and-pregnancy.pdf
